
Introduction: The Four Pillars of Acute Lower Back Strain Relief
Acute lower back strain relief is a critical public health concern, affecting millions of Americans annually. Acute low back pain (LBP) is typically defined as pain lasting less than four weeks and often results from a muscle or ligament strain.
The primary goal of managing any acute lower back strain relief episode is the prompt alleviation of pain and inflammation to allow the patient to regain movement and avoid the risk of chronic pain development. Clinical guidelines in the U.S. generally recommend Over-The-Counter (OTC) analgesics as the first line of pharmacological treatment for non-specific LBP.
Effective management relies on a four-pillar approach, each targeting a different aspect of recovery:
-
Non-Pharmacological Protocols: Strategic use of heat, ice, and movement.
-
Acetaminophen (Tylenol): Analgesia focused on safety and non-inflammatory pain.
-
NSAIDs (Ibuprofen and Naproxen): Potent anti-inflammatory action for acute strains.
-
Optimized Therapies: Topical treatments and combined oral strategies.
This comprehensive guide breaks down the safe dosages, critical side effects, and best practices for achieving effective acute lower back strain relief.
1. Immediate Non-Pharmacological Strategies for Recovery
Before reaching for medication, immediate home interventions can significantly reduce initial discomfort and swelling.
1.1. Safe and effective ways to combine heat and ice for acute back pain
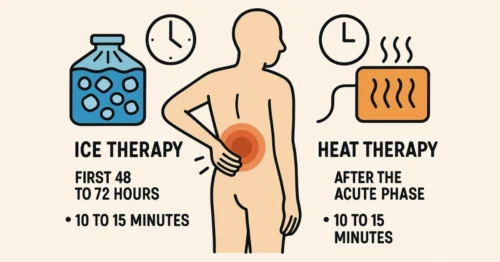
The decision between heat and ice should be based on the timeline of the injury, adhering to a clinically recognized protocol:
-
Ice Therapy (First 48 to 72 Hours): For acute or recent injuries, ice is the preferred choice for the initial 72 hours. Applying ice lowers the body’s temperature in the affected area, reducing inflammation, swelling, and constricting blood vessels. This, in turn, helps to numb the area and decrease the sensation of pain.
-
Usage Protocol: Ice should never be applied for more than 10 to 15 minutes at a time to prevent tissue damage and ensure efficacy.
-
-
Heat Therapy (After the Acute Phase): Once the initial inflammation subsides (typically after 48 to 72 hours), switching to heat therapy is recommended. Heat helps to relax stiff muscles, improve the flexibility of soft tissues, and enhance overall function.
-
Usage Protocol: Heat can be applied on and off for several hours or even days to continue promoting tissue healing. As with ice, application should be limited to 10 to 15 minutes per session to avoid burns.
-
1.2. Does resting the back for too long actually worsen muscle stiffness?
While reducing or stopping normal physical activity for the first few days is necessary to relieve symptoms and reduce swelling, this period of rest must be brief.
Protracted rest (beyond one or two days) can have a detrimental effect, leading to muscle weakness and stiffness. Clinical research emphasizes that gentle, early movement not only aids in acute lower back strain relief but also prevents secondary discomfort and chronic issues. Early return to light activities and stretching (Active Recovery) is a cornerstone of modern physiotherapy, enabling the spine to maintain mobility and support muscle strength.
Want to protect your discs with better seating support?
1.3. Can I use a seat cushion during the initial 48-hour back strain recovery? (SitCushion)
During the critical initial 48-hour recovery period for a back strain, using an ergonomic support, such as a seat cushion, is permissible and often beneficial for comfort, provided the support maintains proper spinal alignment. Products like SitCushion™ can offer improved posture and reduced localized pressure on the lower discs while seated.
Crucial Caveat: Even when using supportive products like SitCushion™, the principle of “Active Recovery” dictates that the user must get up, walk, and gently stretch every 30 to 60 minutes to prevent the very muscle stiffness that prolonged sitting, even with support, can induce.
Transform Your Office Comfort
Sit longer, focus better, and relieve pressure with the SitCushion Office Seat Cushion —
engineered to support your posture and reduce fatigue during long hours at your desk.
2. Pillar 1: Acetaminophen (Tylenol) – Safety-First Pain Relief
Acetaminophen (most commonly Tylenol) is one of the most widely recommended and used OTC analgesics for back pain. Its primary role is pain relief (analgesia), as it does not possess significant anti-inflammatory properties like NSAIDs.
2.1. How much Tylenol (Acetaminophen) can I safely take for acute back pain?
The safety of acetaminophen is directly tied to strict adherence to dosing guidelines, as exceeding the recommended maximum dose can lead to severe and potentially fatal liver toxicity (Hepatotoxicity).
-
FDA Maximum Dose: The maximum total amount of acetaminophen recommended for adults and children 12 years and older should not exceed 4,000 mg in a 24-hour period.
-
Conservative Clinical Caution: While 4,000 mg is the legal maximum, many clinicians advise limiting daily intake to 3,000 mg or less. This safety buffer is crucial because acetaminophen is often hidden in many other OTC and prescription combination products (e.g., cold and flu medicines).
To ensure safe acute lower back strain relief with Tylenol, be aware of the following:
2.2. Critical Side Effects and Risks
The most significant risk associated with acetaminophen is the potential for liver damage (Hepatotoxicity) if the recommended dosage is exceeded. Patients who consume three or more alcoholic drinks daily or have a history of liver disease should severely limit their intake or avoid the drug entirely. In the event of suspected overdose, immediate medical help or contact with Poison Control (1-800-222-1222) is necessary.
3. Pillars 2 & 3: NSAIDs – Targeting Inflammation for Strain Relief
For acute lower back strain relief caused by actual inflammation or muscle strain, Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) such as Ibuprofen and Naproxen are often the most effective choices. These drugs inhibit cyclooxygenase (COX) enzymes, which are responsible for producing the pain- and inflammation-signaling prostaglandins.
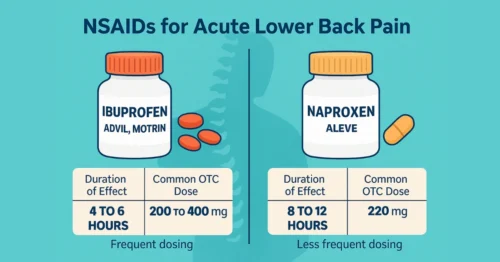
3.1. Should I use Ibuprofen or Naproxen for lower back inflammation?
Both Ibuprofen (Advil, Motrin) and Naproxen (Aleve) are effective for acute lower back strain relief, but they differ significantly in their duration of action, which dictates the clinical choice.
-
Ibuprofen (Ibuprofen for back pain): This is a rapid-onset, short-acting NSAID, providing relief for about 4 to 6 hours. It requires more frequent dosing but offers quick action. The standard OTC adult dosing is 200 to 400 mg every 4 to 6 hours, with a maximum daily OTC dose of 1,200 mg.
-
Naproxen: Naproxen is a longer-acting NSAID, capable of providing pain relief for up to 8 to 12 hours with a single dose. This makes it a superior choice for persistent acute pain, chronic conditions, and for managing pain overnight, as it requires less frequent dosing. The standard OTC dose is 220 mg (1 pill) every 8 to 12 hours, with a maximum of 3 doses (660 mg) in a 24-hour period.
3.2. Critical Safety Profile: Risks of Ibuprofen and Naproxen
NSAID use, particularly if prolonged (beyond a week) or combined with other risks, carries serious side effects:
-
Gastrointestinal Risk: Long-term use significantly increases the risk of stomach ulcers and gastrointestinal bleeding. This risk is higher in older adults or those with a history of stomach issues.
-
Kidney and Cardiovascular Risk: NSAIDs can increase the risk of kidney damage, especially in patients who are dehydrated or have pre-existing kidney dysfunction. Regular, long-term use has also been associated with an increased risk of cardiovascular events.
-
Absolute Warning: Ibuprofen and Naproxen (naproxen vs ibuprofen for back pain), or any other NSAIDs, must never be taken concurrently. Combining them exponentially increases the risk of severe adverse events, especially gastric bleeding and kidney damage, with no added benefit in pain relief.
4. Pillar 4: Optimized and Combined Strategies
For moderate to severe pain, or for patients who cannot tolerate full doses of oral medication, optimized strategies are essential for acute lower back strain relief.
4.1. Topical pain relief options (Diclofenac gel) for targeted back strain
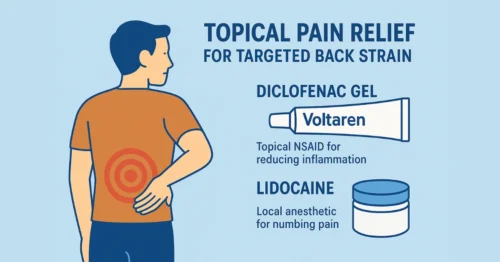
Topical pain relief gels and patches offer a key advantage: they deliver the medication directly to the site of pain, leading to significantly lower systemic (body-wide) absorption and reducing the risk of side effects associated with oral drugs.
-
Diclofenac Gel (Voltaren): This is an OTC topical NSAID. Its mechanism is the same as oral NSAIDs—inhibiting inflammation—but it minimizes the risk of GI and kidney complications.
-
Safe Usage and Dosage: For Diclofenac 1% gel (Voltaren), strict adherence to the dosing card provided with the product is mandatory. The total daily dose across all affected areas should not exceed 32 grams per day. For large muscular areas like the back, the dose must be carefully measured (typically 2g or 4g) and applied up to four times daily.
-
-
Lidocaine: Lidocaine patches or gels act as a local anesthetic, blocking pain signals to the brain. This is an excellent option for patients who prefer not to take oral medication or are seeking targeted relief.
4.2. Dual Therapy: Alternating Acetaminophen and Ibuprofen
For optimal management of moderate-to-severe pain, alternating the use of Acetaminophen and Ibuprofen (Dual Therapy) is a common multimodal strategy. This approach targets different pain pathways—pain relief (Acetaminophen) and inflammation (NSAID)—and helps avoid exceeding the maximum dose of any single drug.
-
Safe Method: The drugs are taken alternately, typically spaced 3 to 6 hours apart, ensuring that the 24-hour maximums for each individual drug are not breached. For example, taking a dose of Acetaminophen (325 mg to 500 mg) and then taking a dose of Ibuprofen (200 mg to 400 mg) three hours later, continuing to alternate.
-
Caution: Due to the complexity of dosing, this strategy should only be undertaken under the guidance of a healthcare professional, especially for patients with kidney, liver, or GI issues.
5. When OTC is Not Enough: Recognizing Warning Signs
Successful acute lower back strain relief requires knowing when self-treatment has reached its limit and professional medical attention is needed.
5.1. When should I switch from OTC medication to a doctor’s evaluation for back pain?
Most acute back strains resolve within a few days to a week with self-care and OTC medication. However, a doctor’s evaluation is necessary if the pain has not improved after approximately one week (7 days) of consistent OTC analgesic use and self-care. Lack of improvement may indicate a deeper issue or a cause not responsive to OTC remedies.
Red Flags – Require Immediate Medical Attention: Certain symptoms suggest a serious underlying condition and warrant immediate medical evaluation:
-
Pain that is severe enough to prevent sleep or the ability to go to work.
-
Pain accompanied by fever, chills, or unexplained weight loss.
-
Pain that progressively radiates down past the knee or causes leg weakness.
-
Loss of bladder or bowel control (This is a medical emergency that can signal cauda equina syndrome, a form of nerve compression).
Want to protect your discs with better seating support?
5.2. Are muscle relaxants like Cyclobenzaprine effective for acute back spasms?
For patients experiencing severe, acute back spasms, prescription muscle relaxants are sometimes considered.
OTC Limitation: There are no over-the-counter muscle relaxants in the United States. Drugs like Cyclobenzaprine (Flexeril) and Carisoprodol (Soma) are prescription-only.
-
Efficacy: Muscle relaxants, particularly Cyclobenzaprine, are effective in decreasing muscle spasms associated with acute musculoskeletal conditions, including back pain. They provide the most benefit in the first few days of therapy.
-
Clinical Role: They are considered alternative or complementary therapy after first- or second-line treatments (like NSAIDs) have failed.
-
Side Effects: They are prescription-only due to adverse effects, primarily significant drowsiness, dizziness, and for some, potential for dependence. These risks necessitate medical supervision, and caution must be used while driving or operating machinery.
6. Frequently Asked Questions (FAQs) for Acute Back Pain Relief
How much Tylenol (Acetaminophen) can I safely take for acute back pain?
The absolute maximum limit set by the FDA for adults is 4,000 mg in a 24-hour period. However, many healthcare professionals recommend limiting the daily dose to 3,000 mg or less to provide a safety buffer, especially considering acetaminophen is an active ingredient in many other OTC cold and flu medications. It is critical to check the labels of all medicines you are taking to ensure you do not exceed this total dose, which can lead to severe liver damage.
Should I use Ibuprofen or Naproxen for lower back inflammation?
Both are Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and are effective at targeting inflammation. The choice depends on your pain pattern:
-
Ibuprofen (e.g., Advil): Provides faster relief but is shorter-acting (4–6 hours). Best for quick, intermittent relief and requires more frequent dosing.
-
Naproxen (e.g., Aleve): Is longer-acting (8–12 hours). This is often preferred for persistent, constant pain or for managing pain overnight, as it requires fewer doses.
Remember, never combine these two drugs, as it significantly increases the risk of side effects like stomach bleeding without providing additional pain relief.
Topical pain relief options (Diclofenac gel) for targeted back strain
Topical treatments like Diclofenac 1% Gel (Voltaren) and Lidocaine patches/gels are excellent choices. Diclofenac is a topical NSAID that is absorbed less systemically than oral pills, thus reducing the risk of gastrointestinal and kidney side effects. Lidocaine acts as a localized anesthetic, blocking pain signals. Diclofenac gel should be carefully measured using the provided dosing card, and the total daily dose should not exceed 32 grams per day across all affected areas.
Are muscle relaxants like Cyclobenzaprine effective for acute back spasms?
Yes, prescription muscle relaxants like Cyclobenzaprine (Flexeril) are effective in decreasing the severe muscle spasms that often accompany acute back strain. However, they are not available OTC and are not considered a first-line treatment. They are typically prescribed for short-term use (up to two weeks) and carry side effects such as severe drowsiness and dizziness, necessitating medical supervision.
When should I switch from OTC medication to a doctor’s evaluation for back pain?
If your back pain has not improved after approximately one week (seven days) of consistent use of OTC pain relievers and self-care, a doctor’s evaluation is warranted. Additionally, seek immediate medical attention if you experience “Red Flag” symptoms, such as severe pain that prevents sleep, pain accompanied by fever, or, most critically, new numbness, weakness in the legs, or loss of bladder or bowel control.
7. Conclusion: A Strategy for Safe and Effective Relief
Achieving optimal acute lower back strain relief requires a strategy that combines timely self-care interventions with strict adherence to safe medication protocols.
By following the four pillars—using ice followed by heat, embracing early, gentle movement (supported by tools like SitCushion™ when seated), and selecting the appropriate OTC pain reliever (Acetaminophen for non-inflammatory pain; Ibuprofen or Naproxen for inflammatory strain)—patients can effectively manage their symptoms. Above all, practicing dosage vigilance (never exceeding 4,000 mg of Acetaminophen or 1,200 mg of OTC Ibuprofen daily) and avoiding the combination of different NSAIDs are paramount for safety. For more in-depth articles on recovery and posture, visit the SitCushion Knowledge Center. To explore supportive solutions for your seating needs during recovery, please see our collection of Seat Cushions. If pain persists beyond one week or is accompanied by neurological red flags, professional medical evaluation is necessary.






