Skip to content
Skip to content 

Executive Summary: The Direct Answer
Orthopedic Seat Cushions serve two distinct functions: ergonomic posture support for low-risk users and clinical skin protection for individuals at risk of pressure injuries. For moderate-risk individuals in home or office settings, high-resiliency (HR) foam or gel-hybrid cushions are recommended to facilitate immersion and manage the skin’s microclimate.
While general-use cushions prioritize spinal alignment and comfort, medical-grade surfaces (HCPCS codes E2603+) must provide superior envelopment to offload bony prominences like the ischial tuberosities. Gel-infused options offer improved thermal regulation, whereas air-cell based systems provide maximum pressure redistribution for high-risk profiles but require rigorous daily maintenance. Effective selection requires balancing a user’s independent weight-shift frequency with a material’s ability to prevent “bottoming out.”
1. Clinical Foundations: The Pathophysiology of Seated Pressure
The prevention of pressure injuries in the seated individual requires a comprehensive understanding of the complex interplay between mechanical force, physiological response, and the environmental factors that comprise the seating interface. According to the National Pressure Injury Advisory Panel (NPIAP), a pressure injury is defined as localized damage to the skin and underlying soft tissue, typically occurring over a bony prominence or related to a medical or other device.
The Mechanisms of Tissue Degradation
The development of these injuries is driven by three major contributors to cellular necrosis: mechanical deformation, inflammation, and ischemia. Research suggests that deformation-induced damage can occur within minutes of exposure to high mechanical loads, as the physical stretching and compression of cell membranes lead to direct structural failure. Ischemia, the restriction of blood flow to the tissues, typically requires a more prolonged exposure of several hours before it manifests as observable tissue death.
The tolerance of soft tissue for these stressors is significantly modulated by the microclimate—the localized temperature and humidity at the skin-support surface interface—as well as nutrition, perfusion, and the presence of co-morbidities such as diabetes or vascular disease. A 1 degree Celsius rise in skin temperature equates to a 13 percent increase in tissue metabolic demand, which accelerates the risk of ischemia when pressure is applied.
NPIAP Pressure Injury Staging
-
Stage 1: Intact skin with localized non-blanchable erythema. Changes in sensation, temperature, or firmness may precede visual cues.
-
Stage 2: Partial-thickness loss of skin with exposed dermis. The wound bed is pink or red and moist.
-
Stage 3: Full-thickness skin loss; adipose tissue is visible. Granulation and rolled edges (epibole) are common.
-
Stage 4: Full-thickness skin and tissue loss with exposed or palpable fascia, muscle, tendon, ligament, or bone.
-
Unstageable: Full-thickness tissue loss in which the extent of damage is obscured by slough or eschar.
-
Deep Tissue (DTPI): Intact or non-intact skin with localized persistent non-blanchable deep red, maroon, or purple discoloration.
2. Biomechanical Engineering: Immersion, Envelopment, and Shear
The efficacy of a seating system is determined by its ability to manage mechanical loads through pressure redistribution. This is primarily achieved through the mechanisms of immersion and envelopment, defined by the Support Surface Standards Initiative (S3I).
The Physics of Redistribution
The relationship between pressure, force, and area is fundamental:
Pressure (P) = Force (F) / Area (A)
As the contact area increases, the pressure exerted on any single point of the tissue decreases, provided the force (body weight) remains constant.
-
Immersion: Refers to the depth to which a body sinks into a support surface.
-
Envelopment: Describes the ability of the surface to conform to the body’s unique shape and irregularities.
Shear and Friction Management
Beyond perpendicular pressure, shear forces represent a critical extrinsic factor. Shear stress is the force per unit area exerted parallel to the skin surface, causing distortion and deformation of the underlying tissues. Friction, the resistance to motion in a parallel direction, often facilitates the development of shear. In the seated position, shear typically occurs when an individual slides forward in the chair or when the backrest is reclined, leading to internal tissue stresses that exceed thresholds for cell survival.
3. Material Science: Air vs. Foam vs. Gel

The selection of a cushion medium is a high-stakes clinical decision that must balance the competing needs for pressure redistribution, postural stability, microclimate management, and durability.
Advanced Polyurethane and High-Resiliency (HR) Foams
Foam cushions remain the foundation of many seating systems due to their reliability and ability to provide structural stability. However, significant differences exist between medical-grade foams and general-use materials.
-
Density: Measured in pounds per cubic foot (pcf) or kilograms per cubic meter (kg/m3), density is the primary indicator of the foam’s durability and ability to resist sagging over time.
-
Indentation Force Deflection (IFD): This measures firmness by determining the force required to compress the material by 25 percent of its original height.
-
High-Resiliency (HR) Foam: Classified by a support factor (the ratio of 65 percent IFD to 25 percent IFD) of 2.4 or higher. This ensures the foam can support significant weight without “bottoming out.”
Gel and Viscous Fluid Systems
Gel and fluid cushions are engineered to mimic the consistency of human fat and muscle tissue, providing superior envelopment for individuals with muscle atrophy.
-
Pros: Highly effective at managing peak interface pressures and reducing shear. Gel’s high thermal mass assists in conducting heat away from the skin.
-
Cons: These cushions are significantly heavier than foam alternatives, which can impact independent transfers. Fluid cushions also require regular “kneading” to prevent gel migration away from high-pressure areas.
Air-Cell Based (ACB) Systems
Air-cell based cushions, utilizing interconnected cells, are the gold standard for high-risk individuals. They allow air to circulate between cells, facilitating deep immersion and extremely low interface pressures.
-
Pros: Superior shock absorption and customized contouring.
-
Cons: Requires high maintenance, including regular pressure checks, and is susceptible to punctures. A leak in an ACB cushion results in immediate bottoming out.
Honeycomb (Thermoplastic Elastomer)
Honeycomb cushions are formed in a matrix pattern, often from thermoplastic urethane.
-
Pros: Lightweight and flexible. The open-cell design provides maximum airflow, making them superior for microclimate control and reducing moisture buildup.
-
Cons: Potential for higher shear forces compared to gel and may not provide adequate pressure relief for individuals with existing severe injuries.
4. Medical-Grade vs. General-Use: A Decision Framework
The clinical distinction between medical-grade cushions and general-use orthopedic cushions is rooted in regulatory oversight, material performance, and the intended environment.
Regulatory and Material Distinctions
Medical-grade cushions are typically FDA-registered and must demonstrate evidence of a quality system (e.g., ISO 13485). They are engineered for aggressive redistribution and feature covers that are fluid-resistant and antimicrobial. General-use orthopedic cushions focus primarily on comfort and ergonomic posture for individuals with intact sensation and mobility. While they may improve spinal alignment, they often lack the immersion depth required for those at high risk of tissue necrosis.
Case Example: SitCushion for Ergonomic Support
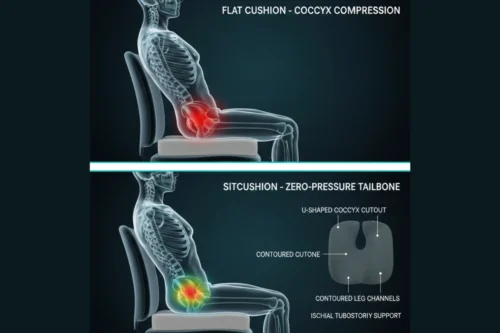
For individuals with mild-to-moderate pressure redistribution needs—such as office workers or drivers—high-specification consumer-grade cushions provide a viable intervention. SitCushion serves as a representative example, utilizing high-density (near 4.8 to 5.0 pcf) precision-molded viscoelastic foam. This material is engineered for a specific hysteresis profile (slow recovery time of 5-10 seconds), which absorbs impact and dampens vibration. The U-shaped coccyx cutout ensures the tailbone floats above the seating surface, redistributing weight to the thighs and glutes. While not a substitute for clinical-grade skin protection in immobile populations, it offers enhanced durability and posture correction for active users.
Medicare/CMS Coding Categories
-
E2601 / E2602 (General Use): Covered for patients with intact skin and low risk who can perform independent weight shifts.
-
E2603 / E2604 (Skin Protection): Required for individuals with a history of pressure injuries or impaired sensation.
-
E2622 / E2624 (Adjustable Skin Protection): Air or fluid systems allowing custom immersion for high-risk users.
5. Standardized Testing: ISO 16840 Metrics
To provide an objective framework for comparing these technologies, the International Organization for Standardization (ISO) developed the 16840 series.
-
ISO 16840-2: Determines physical and mechanical characteristics like immersion and envelopment.
-
ISO 16840-6: Simulated use testing to determine how cushion properties change over time (durability).
-
ISO 16840-13: Assessment of lateral stability, measuring the cushion’s ability to resist the user leaning sideways.
The Impact Damping Test (IDT) is particularly critical; a high-performance cushion must damp impact pulses rapidly to avoid energy transfer to vulnerable tissues during activities such as rolling off a curb.
6. Clinical Decision Matrix
| Risk Level | Mobility Level | Care Setting | Recommended Material |
| Low | Fully mobile; independent shifts | Home / Office | High-Density (HD) Foam |
| Moderate | Active; impaired sensation | Home / Assisted Living | Gel-Foam Hybrid / Viscous Fluid |
| Moderate | Active; high perspiration | Community / Active | Honeycomb (Thermoplastic) |
| High | Immobile; unable to shift | Skilled Nursing / Hospital | Air-Cell Based (ACB) |
| Very High | Total immobility; existing PI | Intensive Care | Alternating Pressure (Active) |
7. Repositioning Protocols: Tilt and Recline
Mechanical repositioning via tilt-in-space systems is a primary preventive intervention for individuals who cannot perform independent weight shifts. These systems redistribute weight away from the ischial tuberosities to the larger surface area of the backrest.
RESNA and NPIAP Guidelines
-
15 degrees or less: No significant advantage for pressure redistribution.
-
25 to 30 degrees: Clinical effectiveness begins.
-
30 to 45 degrees: The optimum range for effective weight shifts and pressure management.
-
Combined Relief: The greatest reduction in pressure is achieved when 25-45 degrees of tilt is used in combination with 110-150 degrees of recline.
Duration and Frequency
Research indicates that a 3-minute duration of tilt and recline is significantly more effective than a 1-minute duration in enhancing skin perfusion. For immobile individuals in chairs, repositioning should occur hourly, whereas high-risk individuals may require offloading every 30 minutes.
8. The Role of Interface Pressure Mapping (IPM)
Interface pressure mapping (IPM) involves a thin, flexible sensor mat placed between the individual and the cushion to quantify pressure distribution.
-
Clinical Utility: IPM identifies “hot spots” of high pressure and helps clinicians compare multiple cushion options for a specific user.
-
Biofeedback: Color-coded maps provide visual cues to users and caregivers on the effectiveness of weight shifts and optimal postural alignment.
-
Limitations: Most systems measure only normal (vertical) forces and cannot quantify shear or friction. IPM reflects a static “snapshot” and may not represent the risks of dynamic activities.
9. FAQ: Seating Comfort and Safety
Q: Can I use a “donut” or ring-shaped cushion for tailbone relief?
A: No. The NPIAP and clinicians explicitly advise against donut cushions. The edges create high-pressure rings that impair circulation and increase edema, often worsening the condition.
Q: How often should I perform a “hand-check”?
A: At least daily. Slide your hand under the cushion core while the user is seated. If there is less than 1 inch of material between the user and the seat base, the cushion has “bottomed out.”
Q: Why does foam density matter?
A: Density determines the durability and lifespan of the foam. High-density foams (40+ kg/m3) resist sagging and maintain their pressure-redistributing properties much longer than lower-density budget foams.
Q: Is memory foam good for pressure relief?
A: Yes, because it provides high levels of immersion and envelopment. However, users should be aware of heat retention and ensure the cushion has a breathable cover.
Professional Disclaimer: This guide is for informational purposes only and does not constitute medical advice. Pressure injury prevention is highly individual. Always consult with a qualified healthcare professional, such as an Occupational Therapist (OT), Physical Therapist (PT), or Assistive Technology Professional (ATP), to undergo a comprehensive seating evaluation before selecting or modifying medical support equipment. Regular skin checks are essential to identify early signs of tissue damage.